Free Medical Examination Louisiana Template
In the heart of ensuring public safety on the road, the Louisiana Department of Public Safety & Corrections Office of Motor Vehicles mandates a comprehensive medical examination for individuals applying for or renewing their driver's licenses, encapsulated in a structured Medical Examination Louisiana form. This form serves as a crucial bridge between the medical assessment of potential drivers and the legal framework guiding the issuance of driving privileges in the state. By requiring a thorough evaluation from a physician, the form highlights various health aspects including orthopedic, hearing, vision, neurological, cardiopulmonary, mental health conditions, diabetes, and more, ensuring that each applicant is physically and mentally equipped to drive safely. The collaborative nature of this process is evident as the form also includes sections for the applicant and the examining physician's attestations, underlining the shared responsibility in promoting road safety. Additionally, the explicit stipulation that failure to complete and return this examination within 30 days will result in the suspension of driving privileges underscores the state’s seriousness about the health and safety of its driving populace. Doctors are provided with legal immunity for their assessments, encouraging candid reporting of impairments that may affect an individual's driving capabilities. Overall, this form acts as a gateway to safe driving, carefully balancing the individual’s right to mobility with the community’s right to safety.
Form Example
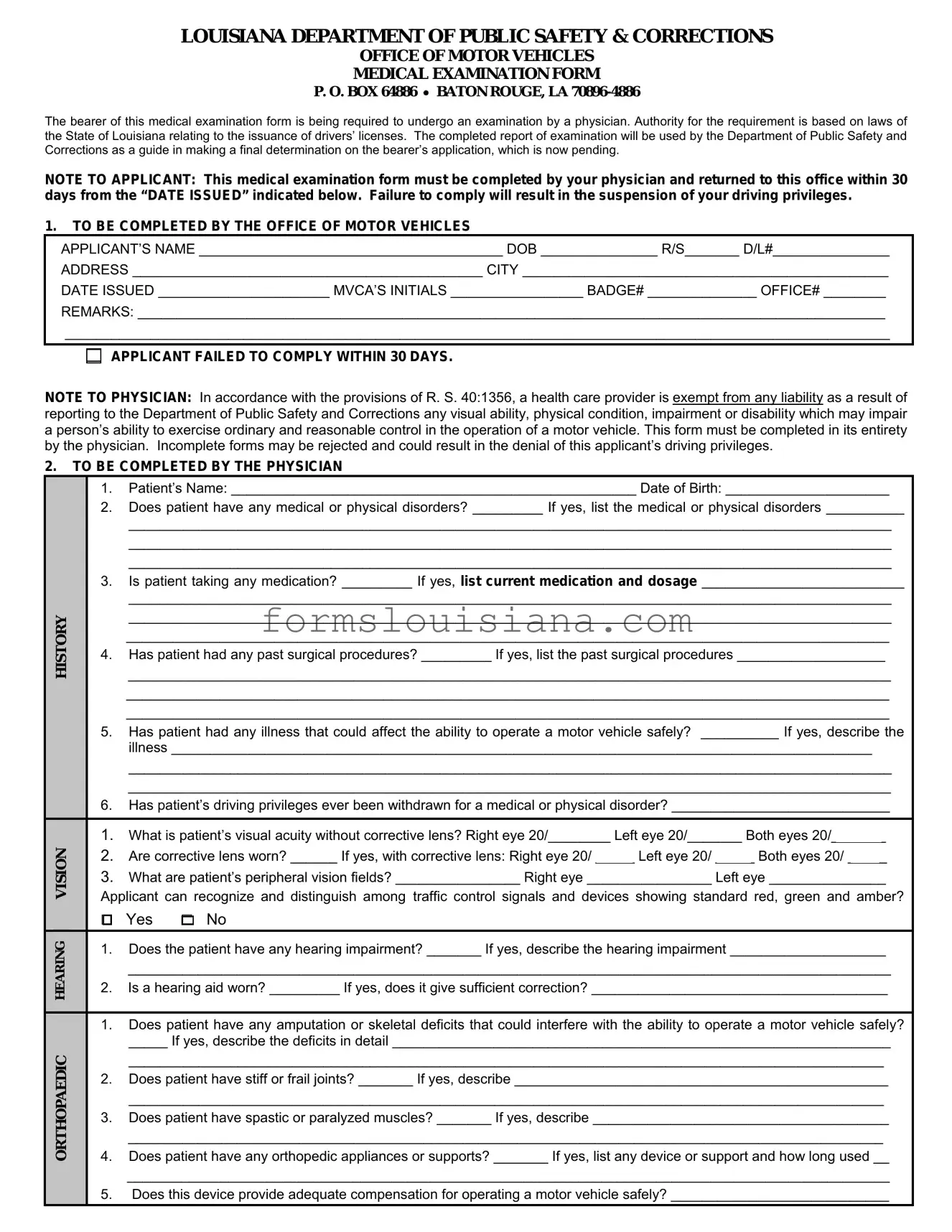
LOUISIANA DEPARTMENT OF PUBLIC SAFETY & CORRECTIONS
OFFICE OF MOTOR VEHICLES
MEDICAL EXAMINATION FORM
P. O. BOX 64886 • BATON ROUGE, LA
The bearer of this medical examination form is being required to undergo an examination by a physician. Authority for the requirement is based on laws of the State of Louisiana relating to the issuance of drivers’ licenses. The completed report of examination will be used by the Department of Public Safety and Corrections as a guide in making a final determination on the bearer’s application, which is now pending.
NOTE TO APPLICANT: This medical examination form must be completed by your physician and returned to this office within 30 days from the “DATE ISSUED” indicated below. Failure to comply will result in the suspension of your driving privileges.
1.TO BE COMPLETED BY THE OFFICE OF MOTOR VEHICLES
APPLICANT’S NAME _______________________________________ DOB _______________ R/S_______ D/L#_______________
ADDRESS _____________________________________________ CITY _______________________________________________
DATE ISSUED ______________________ MVCA’S INITIALS _________________ BADGE# ______________ OFFICE# ________
REMARKS: ________________________________________________________________________________________________
__________________________________________________________________________________________________________
APPLICANT FAILED TO COMPLY WITHIN 30 DAYS.
NOTE TO PHYSICIAN: In accordance with the provisions of R. S. 40:1356, a health care provider is exempt from any liability as a result of reporting to the Department of Public Safety and Corrections any visual ability, physical condition, impairment or disability which may impair a person’s ability to exercise ordinary and reasonable control in the operation of a motor vehicle. This form must be completed in its entirety by the physician. Incomplete forms may be rejected and could result in the denial of this applicant’s driving privileges.
2.TO BE COMPLETED BY THE PHYSICIAN
HISTORY
ORTHOPAEDIC HEARING VISION
1.Patient’s Name: ____________________________________________________ Date of Birth: _____________________
2.Does patient have any medical or physical disorders? _________ If yes, list the medical or physical disorders __________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
3.Is patient taking any medication? _________ If yes, list current medication and dosage __________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
4.Has patient had any past surgical procedures? _________ If yes, list the past surgical procedures ___________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
5.Has patient had any illness that could affect the ability to operate a motor vehicle safely? __________ If yes, describe the illness __________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
6.Has patient’s driving privileges ever been withdrawn for a medical or physical disorder? ____________________________
1.What is patient’s visual acuity without corrective lens? Right eye 20/________ Left eye 20/_______ Both eyes 20/_______
2.Are corrective lens worn? ______ If yes, with corrective lens: Right eye 20/ _____ Left eye 20/ _____ Both eyes 20/ _____
3.What are patient’s peripheral vision fields? ________________ Right eye ________________ Left eye _______________
Applicant can recognize and distinguish among traffic control signals and devices showing standard red, green and amber?
□ Yes □ No
1.Does the patient have any hearing impairment? _______ If yes, describe the hearing impairment ____________________
__________________________________________________________________________________________________
2.Is a hearing aid worn? _________ If yes, does it give sufficient correction? ______________________________________
1.Does patient have any amputation or skeletal deficits that could interfere with the ability to operate a motor vehicle safely?
_____ If yes, describe the deficits in detail ________________________________________________________________
_________________________________________________________________________________________________
2.Does patient have stiff or frail joints? _______ If yes, describe ________________________________________________
_________________________________________________________________________________________________
3.Does patient have spastic or paralyzed muscles? _______ If yes, describe ______________________________________
_________________________________________________________________________________________________
4.Does patient have any orthopedic appliances or supports? _______ If yes, list any device or support and how long used __
__________________________________________________________________________________________________
5.Does this device provide adequate compensation for operating a motor vehicle safely? ____________________________
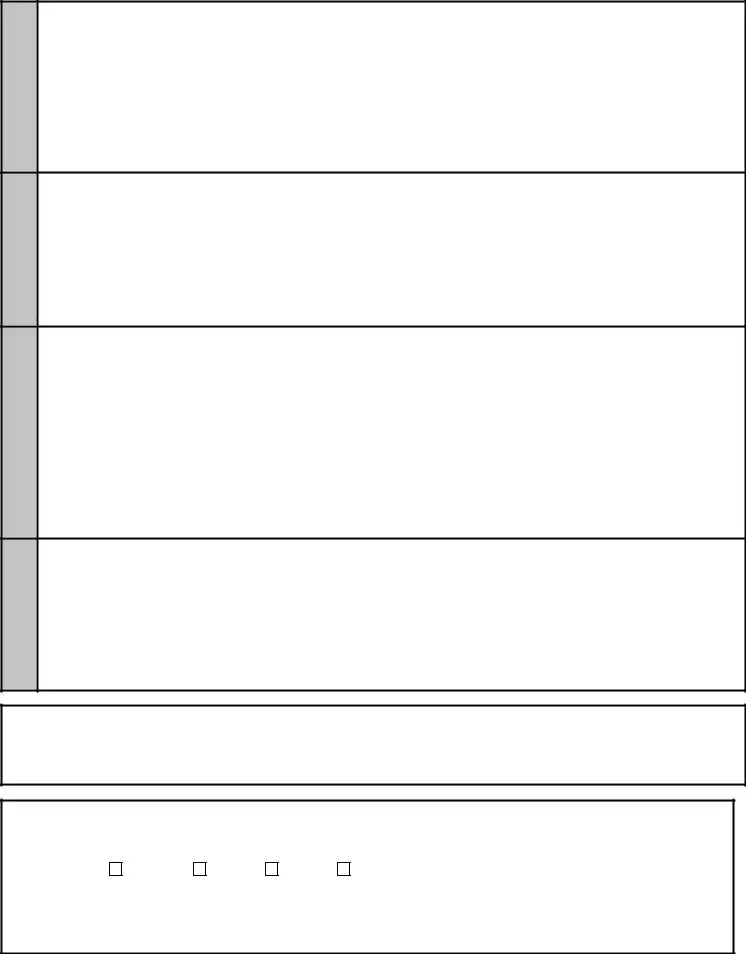
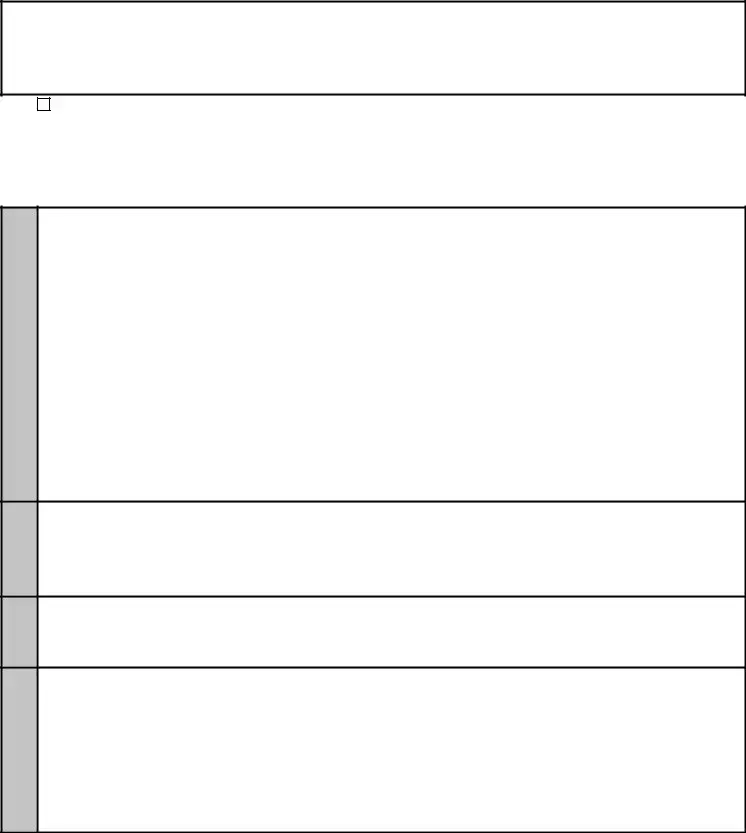
NEUROLOGICAL CARDIOPULMONARY
MENTAL
DIABETES
3.
1.Does patient have angina?______ If yes, when does it occur?_____strenuous activity_____normal activity_____at rest_____
2.Does patient have dyspnea?_____If yes, when does it occur?_____strenuous activity_____normal activity_____at rest_____
3.Does patient have syncope?_____if yes, what is the frequency?__________duration___________last occurance_________
4.Does patient have dizziness?______ describe______________________________________________________________
___________________________________________________________________________________________________
5.What is patient’s blood pressure? 1st reading __________________________ 2nd reading __________________________
6.What is patient’s pulse? Rate __________________________________ Rhythm __________________________________
7.Has patient had cardiovascular catheterization or surgery? ______ If yes, describe _________________________________
___________________________________________________________________________________________________
List medications and dosage: ____________________________________________________________________________
1.Does patient have epilepsy? ______If yes, what type of seizures? _________________ Date of last seizure? ____________
Are seizures completely controlled? _______ Is patient under regular medical care? ________________________________
What are the anticonvulsant serum blood levels? ____________________________________________________________
2.Does patient have any signs of Parkinsonism? ______ If yes, describe condition and severity _________________________
___________________________________________________________________________________________________
Is coordination normal? _______ If no, describe _____________________________________________________________
3.Does patient have any neurological disorder? ______ If yes, describe ___________________________________________
List medications and dosage: ____________________________________________________________________________
Is patient reliable in taking medication and following medical regimen? _____________________________________________
1.Does patient have symptoms of any mental disorder? ______ If yes, describe condition and severity at present ___________
___________________________________________________________________________________________________
2.Has patient ever been treated in a mental hospital? _______ If yes, where and when _______________________________
What was diagnosis and cure? __________________________________________________________________________
3.Does patient use alcohol or drugs? ______ If yes, describe usage ______________________________________________
4.Is patient mentally deficient? ______ If yes, what was highest grade attained in school? ________ age at attainment? _____
5.Does patient have sufficient regard for his/her personal safety as well as that of others to operate a motor vehicle safely? Give details _________________________________________________________________________________________
6.Is patient likely to act on sudden impulse without regard for the consequences of his/her behavior? ____________________
Give details _________________________________________________________________________________________
7.On the basis of your examination and/or knowledge of this patient, do you recommend periodic psychiatric examinations? Give details _________________________________________________________________________________________
List medications and dosage: ____________________________________________________________________________
1.Does patient have a history of diabetes? _______ If yes, is insulin taken? ______ is oral medication taken? ______________
2.What are patient’s laboratory studies? recent urine sugars __________________ recent blood sugars __________________
3.Has patient had any occurrences of diabetic coma? ________ If yes, give dates ___________________________________
4.Has patient had any occurrences of insulin shock? ________ If yes, give dates ____________________________________
5.Does patient have associated abnormalities? visual_______renal_______vascular_______neurological_______other______ If yes, describe _______________________________________________________________________________________
6.Does patient have hypoglycemia? _______ If yes, describe treatment ___________________________________________
List medications taken and dosage: _______________________________________________________________________
Is patient reliable in taking diabetes medication? ______________________ Is diabetes controlled? ______________________
TO BE SIGNED BY PATIENT
I hereby authorize the examining physician whose signature appears below to release all information and findings contained herein to the Louisiana Department of Public Safety and Corrections. The Louisiana Department of Public Safety and Corrections can release this information to such individuals or groups as may be considered necessary and appropriate to determine my ability to safely operate a motor vehicle.
Date _____________________________________ |
Signature of Patient _______________________________________________________ |
4.TO BE COMPLETED, SIGNED AND DATED BY THE PHYSICIAN
PLEASE REFER TO “NOTE TO PHYSICIAN:” on the first page of this form. Are you this patient’s treating physician? _____________
In your opinion, from a medical standpoint, is it safe for this patient to operate a motor vehicle? _______________________________
On the basis of your examination and/or knowledge of this patient, do you recommend periodic medical reports be submitted? _______
If yes, how often? |
6 months |
1 year |
2 years |
other__________ Remarks: ________________________________ |
___________________________________________________________________________________________________________ |
||||
Physician’s Signature _________________________________________________________ Date ___________________________
Physician’s Printed Name ______________________________________________________ Telephone# _____________________
Physician’s Address __________________________________________________________________________________________
DPSMV 2032 (R 04/04)
Document Breakdown
| Fact | Detail |
|---|---|
| Authority Origin | State of Louisiana laws on driver’s license issuance |
| Usage | To guide the Department of Public Safety and Corrections in making a final determination on driving privileges |
| Completion Requirement | Form must be completed by a physician and returned within 30 days from the date issued |
| Non-compliance Consequence | Suspension of driving privileges |
| Physician's Liability Exemption | Exempt from liability for reporting impairments that may affect driving ability (R. S. 40:1356) |
| Form Incompleteness | Incomplete forms may result in the denial of driving privileges |
| Health Conditions Covered | Includes visual ability, physical condition, impairments, disabilities, and medication impacts |
| Patient Authorization Requirement | Patient must authorize release of information to Louisiana Department of Public Safety and Corrections |
Instructions on Filling in Medical Examination Louisiana
Completing the Louisiana Medical Examination Form is a critical step for individuals required to undergo a medical evaluation for driving privileges. This form serves as evidence that the applicant is medically fit to operate a motor vehicle, ensuring the safety of both the applicant and the public. It is important to fill out this form accurately and thoroughly, as incomplete or inaccurate information may lead to delays or denial of driving privileges. Listed below are step-by-step instructions for completing the form.
- Locate the "APPLICANT’S NAME" field and enter your full legal name as it appears on your driver’s license or identification card.
- Fill in your Date of Birth (DOB) in the space provided next to your name.
- Specify your sex (R/S) and Driver's License Number (D/L#).
- Enter your full address, including CITY.
- Note the "DATE ISSUED" as this is the date from when the 30-day period to return this completed form starts.
- Proceed to the section "TO BE COMPLETED BY THE PHYSICIAN." This part is to be filled out by your physician, so ensure that your physician has access to this form during your medical examination.
- Under the "HISTORY" section, your physician must answer questions regarding any medical or physical disorders, medications, past surgical procedures, illnesses that could affect driving, and whether your driving privileges have ever been withdrawn for a medical or physical reason.
- In the "ORTHOPAEDic," "HEARING," and "VISION" sections, your physician is required to provide details about any amputations, skeletal deficits, hearing impairments, and your visual acuity, both with and without corrective lenses.
- The "NEUROLOGICAL," "CARDIOPULMONARY," "MENTAL," and "DIABETES" sections must be completed with detailed information on conditions related to those areas, including but not limited to epilepsy, angina, mental disorders, and diabetes control.
- At the bottom of the form, sign and date the section titled "TO BE SIGNED BY PATIENT," thereby authorizing the physician to release your medical information to the Louisiana Department of Public Safety and Corrections.
- The final section, "TO BE COMPLETED, SIGNED AND DATED BY THE PHYSICIAN," must include the physician’s opinion on whether it is safe for you to operate a motor vehicle, their recommendation on periodical medical reports, their signature, printed name, contact information, and date.
Once the form is fully completed and signed by both the patient and the physician, it should be submitted to the address provided at the top of the form within 30 days from the "DATE ISSUED." Timely submission is essential to avoid the suspension of driving privileges. Remember to keep a copy of the completed form for your records.
Listed Questions and Answers
What is the purpose of the Medical Examination Louisiana form?
The Medical Examination Louisiana form is designed to assess an individual's medical fitness to safely operate a motor vehicle. It's used by the Louisiana Department of Public Safety & Corrections, Office of Motor Vehicles, to make informed decisions regarding the issuance, renewal, or reinstatement of a driver's license. Physicians complete this form to report on a range of medical conditions and their potential impact on driving abilities.
Who needs to complete this form?
This form must be completed by a licensed physician at the request of the Louisiana Office of Motor Vehicles. The form is typically required for individuals who may have medical conditions that could affect their ability to drive safely. The initiating request often comes from the Department of Public Safety & Corrections based on specific criteria or concerns regarding an applicant's health and driving capabilities.
What happens if the form is not returned within 30 days?
If the completed Medical Examination form is not returned to the Office of Motor Vehicles within 30 days from the date it was issued, the applicant's driving privileges may be suspended. Timely submission is crucial to avoid the suspension of driving rights.
What kind of medical information does the form require?
The form requests detailed medical information across various sections, including:
- History of medical or physical disorders
- Current medications and dosages
- Details of past surgical procedures
- Any illnesses affecting safe driving
- Visual and hearing acuity
- Orthopaedic, cardiopulmonary, neurological, mental health, and diabetes information
This comprehensive medical evaluation helps determine if an individual can maintain ordinary and reasonable control over a motor vehicle.
Is there any liability for physicians who report medical conditions?
No, physicians are exempt from liability for reporting a person’s medical conditions to the Department of Public Safety and Corrections. This is in accordance with R.S. 40:1356, which is aimed at ensuring public safety on the roads.
What instructions are given to physicians?
Physicians are instructed to complete the form in its entirety, providing detailed information on the patient’s medical condition, medications, and any other factors that might affect their ability to drive. Incomplete forms may lead to the rejection of the application and denial of driving privileges. This ensures that a thorough and accurate assessment is made regarding a patient's fitness to drive.
What does the vision section entail?
In the vision section, physicians must report the patient's visual acuity with and without corrective lenses for each eye and both eyes together, as well as peripheral vision fields. They must also confirm whether the patient can recognize and distinguish between standard traffic signals and devices.
What are the consequences of failing to report a medical condition?
Failure to accurately report a medical condition that could impair driving can lead to the patient inadvertently being allowed to drive when it may not be safe to do so. This can pose a significant risk to public safety and potentially result in legal repercussions for the driver if they are involved in an accident.
Can the form be used against a driver to revoke driving privileges?
Yes, if the medical examination reveals that a driver is medically unfit to safely operate a motor vehicle due to a physical or mental condition, the Department of Public Safety & Corrections may use the information to revoke or suspend the driver's license. The primary goal is to ensure that all drivers on the road have the necessary physical and mental capabilities to drive safely.
How often must this form be submitted?
The necessity to submit this form is generally determined on a case-by-case basis, often initiated by the Office of Motor Vehicles in response to specific concerns about a driver's health. Additionally, the physician may recommend periodic medical reports, suggesting intervals like every 6 months, 1 year, or 2 years, depending on the nature of the medical condition and its potential impact on driving ability.
Common mistakes
- Not reviewing the form for completeness before submission: Every section of the form must be filled out accurately. Missing information can result in delays or the rejection of the application.
- Overlooking the detail in the instructions: Both the applicant and the physician must pay close attention to the specific instructions provided at the beginning of the form. These instructions guide how each section should be completed and the importance of thoroughness cannot be overstated.
Failing to accurately report medical conditions:
It's crucial that all medical or physical disorders, medications, and any surgical history that could affect driving abilities are fully disclosed. Omissions or inaccuracies can have serious implications.Not updating personal information:
Applicants must ensure that all personal information, including their address and contact details, is current and accurate. This information is essential for the Department of Public Safety and Corrections to maintain proper communication.Misunderstanding the deadline: The form stipulates that it must be completed and returned within 30 days from the "DATE ISSUED". Missing this deadline can result in the suspension of driving privileges, a detail that is critically important yet often overlooked.
Forgetting to sign the document:
The form requires signatures from both the patient and the physician. An unsigned document is considered incomplete and will not be processed.
Documents used along the form
When undergoing a medical examination in Louisiana for the purpose of obtaining or renewing a driver’s license, various other documents and forms might be required or helpful alongside the Medical Examination Louisiana form to ensure a comprehensive assessment of an individual's ability to safely operate a motor vehicle. These documents support a thorough understanding of an individual's health status and any accommodations or restrictions that may need to be applied to their driving privileges.
- Vision Examination Report: This form assesses an individual's eyesight to ensure it meets the state's driving standards. It details the level of visual acuity, field of vision, and any need for corrective lenses.
- Proof of Identity and Residency Documents: These are essential for all drivers looking to obtain or renew their license in Louisiana, including a birth certificate, passport, and/or utility bills, to establish identity and residency within the state.
- Driver’s License Application Form: A completed application form is necessary for new drivers or existing drivers seeking renewal. It gathers personal information, driving history, and might include consent for the Department of Public Safety and Corrections to run background checks.
- Medical History Form: A detailed medical history provides context to the physician conducting the medical examination, highlighting past conditions, surgeries, or ongoing health issues that might affect driving abilities.
- Medication List: A current list of medications including dosages, prescribed by health care providers, helps in assessing any potential side effects or impairments to motor skills or cognitive functions critical for safe driving.
- Consent for Release of Information: This form authorizes the Department of Public Safety and Corrections to obtain medical records or information from healthcare providers, necessary for evaluating driving capacities.
- Driver’s Self-Certification of Medical Fitness Form: Some drivers, especially those with commercial licenses, may be required to self-certify their medical fitness for driving, indicating any medical conditions that could interfere with safe operation of a vehicle.
The integration of these documents with the Medical Examination Louisiana form enables a holistic evaluation of a person's fitness to drive, addressing medical conditions that could impact driving safety. It is important for individuals required to complete these forms to provide accurate and comprehensive information to avoid potential legal issues or endangerment to themselves and other road users.
Similar forms
The Medical Examination Louisiana form is similar to various other health declaration documents used across different sectors and states for verifying individuals' health status for specific purposes, such as employment, vehicle operation, and more. Each document, while serving distinct objectives, aligns on the core requirement of detailed health examination results performed by authorized medical personnel.
One such document is the Department of Transportation (DOT) Medical Examination Report utilized nationwide. Like the Louisiana form, the DOT Medical Examination Report mandates a thorough health check by a licensed medical examiner listed on the National Registry of Certified Medical Examiners. This report evaluates an individual’s physical qualifications to safely operate commercial motor vehicles. Both documents focus on assessing an applicant’s physical abilities, sight and hearing capabilities, and overall health condition to ensure public safety on the roads. The emphasis is particularly on conditions that could impair driving, such as cardiovascular health, neurological disorders, and diabetes management.
Another analogous document is the Federal Aviation Administration (FAA) Medical Certificate. Pilots are required to obtain this certification, which involves a comprehensive medical examination similar to the one detailed in the Louisiana medical examination form. The FAA Medical Certificate assesses the applicant's vision, hearing, cardiovascular health, and mental health status, among other criteria. Although it is for aviating rather than driving, the focus on ensuring the individual does not possess any medical conditions that could compromise safety is a common denominator shared with the Louisiana vehicle operator's health assessment.
The Pre-Employment Physical Examination forms used by various employers also share similarities with the Medical Examination Louisiana form. These forms are designed to ascertain if an applicant is medically and physically capable of handling the tasks associated with a job offer. While the specifics of these examinations vary depending on the nature of the job, they commonly include checks on physical abilities, chronic illnesses, vision and hearing tests, and sometimes mental health assessments. This parallels the Louisiana form’s purpose of ensuring an individual's health status does not pose a risk to public safety, especially when operating a motor vehicle.
Each of these documents, whether for driving commercial vehicles, flying aircraft, or performing job-related tasks, underscores the importance of maintaining high standards of health and safety. They reflect a collective commitment to public welfare, demanding rigorous health scrutiny to prevent accidents or incidents caused by medical conditions. Despite the varying contexts in which they are used, the core philosophy of safeguarding lives through comprehensive medical evaluation remains consistent.
Dos and Don'ts
When it comes to filling out the Medical Examination Form for the Louisiana Department of Public Safety & Corrections, Office of Motor Vehicles, there are specific dos and don'ts that can help ensure the process is smooth and successful. Below is a list of guidelines to follow:
- Do ensure that the form is completed by a licensed physician. This is a mandatory requirement as the assessment needs to be medically accurate.
- Do double-check that all parts of the form are filled out. Incomplete forms can lead to delays or the denial of the application for driving privileges.
- Do list all medical or physical disorders truthfully. Full disclosure is essential for a fair evaluation of the ability to safely operate a motor vehicle.
- Do include a comprehensive list of medications and dosages currently being taken. This information helps in assessing overall health and any potential impacts on driving ability.
- Don't forget to report any history of surgical procedures, illness, or any condition that could affect driving safety. This includes both past and present conditions.
- Don't leave out details about any supportive devices or aids used, including hearing aids, orthopedic supports, or corrective lenses. These are important in evaluating driving capabilities.
- Don't omit information about any psychiatric conditions or treatments. Mental health is equally important as physical health in assessing safe driving.
- Don't delay in submitting the completed form within the 30-day timeframe. Late submissions can result in the suspension of driving privileges.
Misconceptions
There are several misconceptions surrounding the Medical Examination Louisiana form that can lead to confusion or misunderstanding. It's important to clarify these misconceptions to ensure individuals are fully informed about the process and requirements.
- Only for Driver’s License Application: Some people believe that the Medical Examination Louisiana form is exclusively for new driver’s license applications. However, this form may also be required for license renewals or reinstatements for individuals with certain medical conditions that could affect their driving ability.
- Any Doctor Can Sign: A common misconception is that any healthcare provider can complete and sign the form. In reality, the form must be completed by a licensed physician who is familiar with the patient’s medical history and current condition.
- One-Time Requirement: Many assume that once submitted, the medical examination is a one-time requirement. The truth is, depending on the physician’s recommendations and the nature of the medical condition, periodic re-examinations may be required to ensure ongoing fitness to drive.
- Privacy Concerns: Individuals often worry about privacy violations with the submission of this form. It's important to note that the information provided is used solely to assess the individual’s ability to safely operate a motor vehicle and is protected under privacy laws.
- Limited to Physical Health: There’s a misconception that the form only assesses physical health. In fact, it covers a broad spectrum of health considerations, including vision, hearing, mental health, and neurological conditions that could impair driving.
- No Liability for Physicians: Some believe that physicians may face liability for reporting health conditions to the Department of Public Safety and Corrections. The form explicitly states that healthcare providers are exempt from liability for reporting impairments that may affect driving abilities.
- Immediate Suspension of Driving Privileges: A final misconception is that failing to submit the form will result in an immediate and permanent suspension of driving privileges. While failure to comply within the given timeframe can lead to suspension, individuals typically have the opportunity to submit the form late or appeal the suspension to regain their driving abilities.
Understanding these aspects of the Medical Examination Louisiana form is crucial for individuals undergoing the medical examination process. Clearing up these misconceptions helps in navigating the procedure more effectively and ensures compliance with state regulations for maintaining or re-establishing driving privileges.
Key takeaways
Filling out the Medical Examination Louisiana form is a crucial step for individuals required to undergo a medical examination for their driver’s license in Louisiana. Here are the key takeaways for both applicants and physicians involved in the process:
- The form is issued by the Louisiana Department of Public Safety & Corrections, Office of Motor Vehicles, and serves as a tool for assessing an applicant's medical fitness to drive.
- Applicants must have the form completed by a licensed physician and returned to the Office of Motor Vehicles within 30 days from the date issued to avoid suspension of driving privileges.
- The medical examination covers various areas including orthopedic, hearing, vision, neurological, cardiopulmonary, mental health, and diabetes assessments to ensure comprehensive evaluation.
- Physicians are reminded that according to R.S. 40:1356, they are exempt from liability for reporting any conditions that may impair the patient's ability to safely operate a vehicle.
- Incomplete forms may be rejected, potentially leading to the denial of the applicant's driving privileges, highlighting the importance of thorough completion.
- Questions in the form address both current and historical health issues, medications, and surgical procedures that could influence driving abilities, emphasizing the need for honest and detailed answers.
- Patients are required to authorize their examining physician to release all findings to the Louisiana Department of Public Safety and Corrections, which underscores the confidentiality and seriousness of the form.
- The physician’s section includes a crucial question about the patient’s medical fitness for driving, and whether periodic medical reports should be submitted, guiding the Department's final decision on the applicant's license status.
Proper completion and timely submission of the Medical Examination Louisiana form are essential steps in the process of evaluating an individual's capability to operate a motor vehicle safely. It serves as a bridge between health concerns and public safety, ensuring that only those fit to drive are legally allowed to do so.
Popular PDF Templates
Louisiana 2022 Tax Forms - A pivotal resource for ensuring your requests to Louisiana state agencies are submitted properly and promptly.
Louisiana State Income Tax Forms - Allows for detailed calculation of Louisiana income tax, including adjustments based on federal income and applicable state credits.