Free Louisiana Medicaid Freedom of Choice List Template
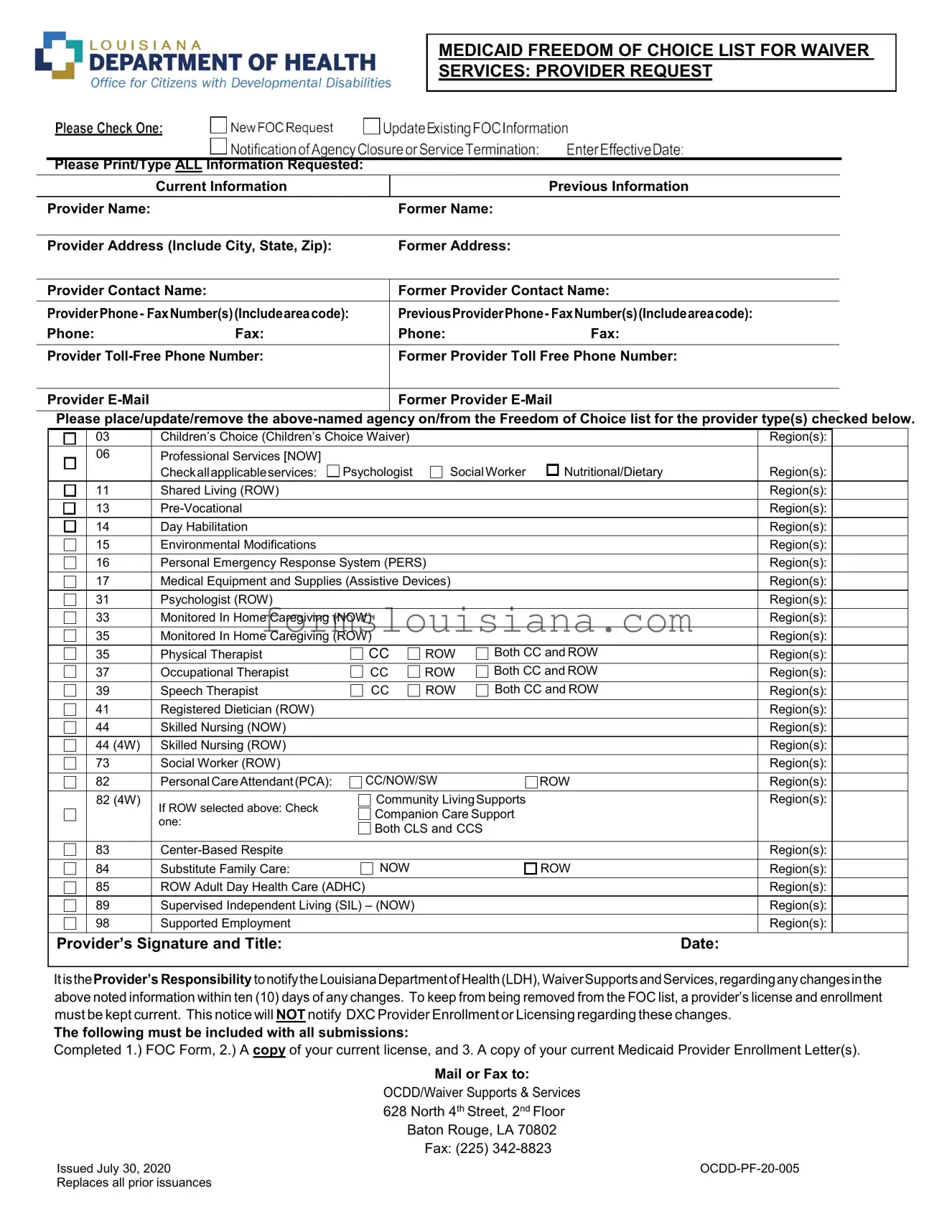
The Louisiana Medicaid Freedom of Choice List form is a critical document intended for providers offering waiver services under Medicaid, aiming to ensure that Medicaid recipients have the freedom to choose among a variety of providers for their healthcare needs. This form facilitates the inclusion, update, or removal of provider information on the Freedom of Choice (FOC) list, capturing essential details such as current and previous provider information, contact names, phone and fax numbers, and email addresses. Providers can specify the types of services they offer, including a wide range of categories from psychological services, nutritional/dietary guidance, to skilled nursing and personal emergency response systems, across different Medicaid waivers such as Children's Choice, NOW, and ROW. This form not only mandates the completion and submission of current licensing and Medicaid Provider Enrollment Letters but also emphasizes the provider’s responsibility to inform the Louisiana Department of Health (LDH) about any changes to their information within ten days to maintain their status on the FOC list. Issued on July 30, 2020, the form underscores the importance of accurate and up-to-date information to ensure continuous service provision to Medicaid beneficiaries without disruption, reflecting the dynamic nature of healthcare service provision and the need for timely communication between providers and the LDH.
Form Example
MEDICAID FREEDOM OF CHOICE LIST FOR WAIVER
SERVICES: PROVIDER REQUEST
Please Print/Type ALL Information Requested:
|
Current Information |
|
Previous Information |
|
|
|
|
Provider Name: |
|
Former Name: |
|
|
|
|
|
Provider Address (Include City, State, Zip): |
Former Address: |
|
|
|
|
||
Provider Contact Name: |
Former Provider Contact Name: |
||
|
|
||
ProviderPhone- FaxNumber(s)(Includeareacode): |
PreviousProviderPhone- FaxNumber(s)(Includeareacode): |
||
Phone: |
Fax: |
Phone: |
Fax: |
|
|
||
Provider |
Former Provider Toll Free Phone Number: |
||
|
|
|
|
Provider |
|
Former Provider |
|
|
|
|
|
Please place/update/remove the
|
03 |
Children’s Choice (Children’s Choice Waiver) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
06 |
Professional Services [NOW] |
|
|
|
|
|
|
|
|
|
Checkallapplicableservices: |
Psychologist |
SocialWorker |
Nutritional/Dietary |
|
Region(s): |
|
|
|
11 |
Shared Living (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
Region(s): |
|
|
|
14 |
Day Habilitation |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
Environmental Modifications |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
||
|
16 |
Personal Emergency Response System (PERS) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
||
|
17 |
Medical Equipment and Supplies (Assistive Devices) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
|
|
|
31 |
Psychologist (ROW) |
|
|
|
|
|
Region(s): |
|
|
33 |
Monitored In Home Caregiving (NOW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Monitored In Home Caregiving (ROW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Physical Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
37 |
Occupational Therapist |
CC |
ROW |
Both CC and ROW |
|
: |
|
|
|
|
|
|
Region(s) |
|
||||
|
39 |
Speech Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
41 |
Registered Dietician (ROW) |
|
|
|
|
|
Region(s): |
|
|
44 |
Skilled Nursing (NOW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
44 (4W) |
Skilled Nursing (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
73 |
Social Worker (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
82 |
Personal CareAttendant(PCA): |
CC/NOW/SW |
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
||
|
82 (4W) |
If ROW selected above: Check |
Community LivingSupports |
|
|
Region(s): |
|
||
|
|
Companion Care Support |
|
|
|
|
|||
|
|
one: |
|
|
|
|
|||
|
|
Both CLS and CCS |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
83 |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
84 |
Substitute Family Care: |
NOW |
|
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
85 |
ROW Adult Day Health Care (ADHC) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
89 |
Supervised Independent Living (SIL) – (NOW) |
|
|
|
|
Region(s): |
|
|
|
98 |
Supported Employment |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
Provider’s Signature and Title: |
|
|
|
|
Date: |
||||
|
|
|
|
|
|
|
|
|
|
ItistheProvider’s Responsibility tonotifytheLouisianaDepartmentofHealth(LDH),WaiverSupportsandServices,regardinganychangesinthe above noted information within ten (10) days of any changes. To keep from being removed from the FOC list, a provider’s license and enrollment must be kept current. This notice will NOT notify DXC Provider Enrollment or Licensing regarding these changes.
The following must be included with all submissions:
Completed 1.) FOC Form, 2.) A copy of your current license, and 3. A copy of your current Medicaid Provider Enrollment Letter(s).
Mail or Fax to:
OCDD/Waiver Supports & Services
628North 4th Street, 2nd Floor Baton Rouge, LA 70802 Fax: (225)
Issued July 30, 2020 |
|
Replaces all prior issuances |
|
Document Breakdown
| # | Fact |
|---|---|
| 1 | The Louisiana Medicaid Freedom of Choice List form is used to add, update, or remove a provider's information on the Freedom of Choice (FOC) list for waiver services. |
| 2 | Providers must print or type all requested information, including current and previous information regarding names, addresses, contact details, and services offered. |
| 3 | The form is specific to several types of waiver services such as Children’s Choice, Professional Services, Shared Living, and others, allowing providers to specify the regions and services they offer. |
| 4 | Providers are responsible for notifying the Louisiana Department of Health (LDH), Waiver Supports, and Services about any changes to the information provided on the form within ten days to avoid being removed from the FOC list. |
| 5 | To submit the form, providers must include a signed FOC form, a copy of their current license, and a copy of their current Medicaid Provider Enrollment Letter(s). |
| 6 | Submissions can be mailed or faxed to the Office for Citizens with Developmental Disabilities (OCDD)/Waiver Supports & Services in Baton Rouge, LA. |
| 7 | The form, identified as OCDD-PF-20-005, issued on July 30, 2020, replaces all prior issuances, emphasizing the importance of using the latest version for compliance. |
Instructions on Filling in Louisiana Medicaid Freedom of Choice List
Filling out the Louisiana Medicaid Freedom of Choice List form is a straightforward process but requires attention to detail. This form is essential for providers who wish to offer waiver services under Louisiana's Medicaid program. It includes updating information about provider services and ensuring that Medicaid participants have the freedom to choose from a list of qualified providers. The form requires both current and, if applicable, previous information about the provider, as well as details about the services they are offering. Careful completion and timely submission of this form, alongside required documents, ensure that providers can continue to deliver services without interruption.
- Start by printing or typing all the requested information at the top of the form. Include both the current and, if applicable, the former names, addresses, contact names, phone and fax numbers, and email addresses for the provider.
- In the section labeled "Please place/update/remove the above-named agency on/from the Freedom of Choice list for the provider type(s) checked below," check the appropriate box(es) to indicate whether you are adding, updating, or removing the provider's information.
- Select the waiver service types you are requesting to provide. These services are listed with checkboxes - make sure to check all that apply. Indicate the regions in which you plan to offer these services.
- For services that offer options like "CC" (Children's Choice), "NOW" (New Opportunities Waiver), "ROW" (Residential Options Waiver), or both, ensure to select the appropriate checkbox to indicate the specific waiver program(s) your services will be associated with.
- Sign and date the form at the bottom where it says, "Provider’s Signature and Title." Ensure the date is correct to avoid any processing delays.
- Review the form to ensure all the information provided is accurate and complete. Accuracy is critical to avoid any delays in processing or potential issues with being listed correctly in the Freedom of Choice list.
- Collect the necessary documents to be submitted along with the form. These include:
- A completed Freedom of Choice (FOC) Form.
- A copy of your current license relevant to the services you are providing.
- A copy of your current Medicaid Provider Enrollment Letter(s).
- Mail or fax the completed form and accompanying documents to the address or fax number provided: OCDD/Waiver Supports & Services, 628 North 4th Street, 2nd Floor, Baton Rouge, LA 70802. Fax: (225) 342-8823.
- Keep a copy of all submitted documents for your records. Having a record will be helpful for any future references or in case further communication with the Louisiana Department of Health is needed.
Upon submission, the Louisiana Department of Health (LDH) Waiver Supports and Services will process the information. The provider is responsible for notifying the LDH of any changes in the provided information within ten days of making such changes. To remain on the Freedom of Choice list, maintaining a current license and provider enrollment is crucial. It's important to note that this process does not notify DXC Provider Enrollment or Licensing regarding these changes, so separate communication may be required for updating those entities.
Listed Questions and Answers
What is the Louisiana Medicaid Freedom of Choice List form?
The Louisiana Medicaid Freedom of Choice List form is a document used by healthcare providers to request listing on, update information for, or be removed from the choice list that Medicaid recipients use to select waiver service providers. It's essential for keeping provider information current and ensuring Medicaid recipients have access to the latest provider choices for various services.
Who needs to complete this form?
Healthcare providers offering services under Louisiana Medicaid waiver programs need to complete this form. This includes new providers who wish to be listed and existing providers who need to update or change their information, or who want to be removed from the list.
What types of services can be listed on the form?
Providers can check off a variety of services on the form, including but not limited to:
- Children’s Choice Waiver Services
- Professional Services such as Psychological and Social Work Services
- Day Habilitation and Pre-Vocational Services
- Medical Equipment and Supplies
- Personal Care Attendant Services
- Adult Day Health Care
- Supported Employment Services
What information is required to fill out the form?
The form requires both current and previous provider information if applicable, including:
- Provider's name and former name (if any)
- Address and previous address
- Contact name
- Phone and fax numbers, including toll-free numbers
- Email address
How does a provider submit the form?
The completed form, along with a copy of the provider's current license and Medicaid Provider Enrollment Letter(s), should be mailed or faxed to OCDD/Waiver Supports & Services at the address or fax number provided on the form.
What happens after submitting the form?
After submission, the provider's information will be updated on the Medicaid Freedom of Choice list as requested, making it available to Medicaid recipients looking for waiver services. Providers are responsible for informing the Louisiana Department of Health about any future changes.
Is there a deadline for submitting updates or changes?
Yes, providers must notify the Louisiana Department of Health within ten days of any changes to their information to maintain their listing on the Freedom of Choice list without interruption.
What is the significance of keeping a license and enrollment up to date?
Maintaining an up-to-date license and Medicaid enrollment is crucial to remain on the Freedom of Choice list. Providers with outdated information risk being removed from the list, which can affect Medicaid recipients’ access to their services.
Common mistakes
Filling out the Louisiana Medicaid Freedom of Choice List form is a necessary step for providers offering waiver services. However, mistakes can happen. Here are seven common ones:
- Not printing or typing clearly: All information requested on the form should be printed or typed to ensure legibility. Illegible handwriting can cause delays or result in incorrect data being recorded.
- Omitting current or previous information: It's essential to complete both the current and previous sections for provider information. Skipping any fields may lead to incomplete documentation.
- Inaccurate provider type selections: The form contains multiple provider types and services checkboxes. Selecting incorrect types or services can mislead the allocation processes and affect the provider's ability to deliver appropriate care.
- Failure to check applicable regions: For each service provided, the relevant regions must be checked. Neglecting to specify these can limit the provider's service delivery to the appropriate geographic areas.
- Forgetting to sign and date the form: The provider's signature and the date are crucial for validating the request. An unsigned or undated form is typically considered incomplete and can be rejected.
- Not including required attachments: The form requires accompanying documents, such as a current license and a current Medicaid Provider Enrollment Letter. Failing to attach these can halt the process.
- Failing to notify of changes within ten days: Providers must inform the Louisiana Department of Health about any information changes within ten days. Overlooking this responsibility can lead to removal from the Freedom of Choice list.
To ensure a smooth registration or update process, providers are encouraged to double-check their form before submission, focusing on clear and complete entries, accurate selections, and adherence to all specified requirements.
Documents used along the form
When navigating the complexities of Louisiana Medicaid, especially regarding waiver services and provider options, an assortment of crucial forms and documents come into play alongside the Louisiana Medicaid Freedom of Choice (FOC) List form. These items are essential for both providers seeking to join the Medicaid network and beneficiaries selecting their services.
- Provider Enrollment Application: A primary document required for healthcare providers to become a recognized Medicaid provider, detailing personal and professional credentials that must be verified.
- Current License Proof: Providers must submit a copy of their current professional license, ensuring they meet state standards for the services they offer.
- Medicaid Provider Enrollment Letter: This letter confirms a provider's enrollment in the Medicaid program, a necessary step before they can be listed on the FOC.
- Service Agreement Form: Details the specific services a provider agrees to offer to Medicaid beneficiaries, including limitations and conditions of service.
- Beneficiary Selection Form: Used by Medicaid recipients to select or change their provider under waiver programs, ensuring their right to choose.
- Provider Update Form: Essential for current providers to inform Medicaid of changes in services, contact information, or location to maintain accurate listings and ensure compliance.
- Health Risk Screening Tool: Deployed to assess individual care needs of beneficiaries, determining the level and type of services required.
- Incident Report Form: A form required to report any unusual or unexpected incidents affecting beneficiaries under care, ensuring transparency and accountability.
Together, these documents constitute a comprehensive framework that supports the integrity and functionality of the Louisiana Medicaid program. They ensure that providers are properly credentified and services are delivered effectively to meet the diverse needs of beneficiaries. From initial provider enrollment to ongoing service delivery, each document plays a crucial role in facilitating a fluid, transparent, and equitable healthcare system for Louisiana's Medicaid population.
Similar forms
The Louisiana Medicaid Freedom of Choice List form is similar to several other key documents in the healthcare sector, each serving specific but occasionally overlapping purposes. These documents facilitate a structured way for healthcare providers to communicate with governmental or regulatory bodies about their services, qualifications, and changes in their service offerings or locations.
The National Provider Identifier (NPI) Application/Update Form bears resemblance to the Louisiana Medicaid Freedom of Choice List form, in that both are used by healthcare providers to register or update their practice information. The NPI form is critical for all healthcare providers in the United States as it collects their identifying information, practice locations, and specialty information for inclusion in a national registry. This registry is accessed by insurers and patients alike to verify provider credentials. Similarly, the Louisiana form is crucial for Medicaid providers in Louisiana to be enlisted or to update their details for Medicaid services, specifically those requiring waiver services.
The Provider Enrollment Application for Medicare is another document with similarities to the Louisiana Medicaid Freedom of Choice List form. Both documents are integral for providers who wish to engage with government-funded healthcare programs, be it Medicare or Medicaid. While the Provider Enrollment Application allows healthcare providers to submit their credentials to be able to bill Medicare for their services, the Louisiana Medicaid form specifically deals with the providers' ability to offer services under Medicaid waivers. Each of these forms ensures the provider's information is current and accurately reflected in their respective healthcare programs, safeguarding patients' access to verified and qualified providers.
Change of Information forms for state professional licensing boards also share commonalities with the Louisiana Medicaid Freedom of Choice List form. Professional healthcare providers are required to maintain current information with their state's professional licensing board, such as changes in addresses, contact information, or services offered. These forms, like the Louisiana Medicaid form, are necessary for the ongoing assurance of a provider's credibility and reliability in their professional practice. Ensuring this information is current assists in maintaining a trustworthy healthcare system where providers are easily accessible and verifiable by both regulatory bodies and the public.
Dos and Don'ts
- Ensure that all the requested information is printed or typed clearly to avoid any misunderstandings or processing delays.
- Double-check that the provider name, both current and former if applicable, along with the address details are accurate and fully updated to reflect any recent changes.
- For the section that requests updates on the Freedom of Choice list for provider types, carefully check all applicable services you provide and the regions you serve to ensure your listing is accurate.
- Include a copy of your current license and a copy of your current Medicaid Provider Enrollment Letter(s) with the submission to meet all requirements for processing.
- Sign and date the form. Remember, the responsibility to inform the Louisiana Department of Health regarding any changes within ten days falls on the provider. This is crucial to avoid being removed from the Freedom of Choice list because of outdated information.
Things to Do:
- Do not leave any requested fields blank. If a section does not apply, write “N/A” to indicate that the question has been considered but is not applicable.
- Avoid using unclear handwriting if filling out the form manually. Misinterpretations due to illegibility can lead to incorrect information being processed.
- Do not forget to include the requested attachments (your current license and Medicaid Provider Enrollment Letter(s)). Failing to include these documents can result in delays or rejection of your request.
- Refrain from waiting until the last minute to notify the Louisiana Department of Health about changes in your information. Late notifications can put your listing at risk.
- Do not ignore the requirement to sign and date the form. An unsigned or undated form is often considered incomplete and can be grounds for delay or non-acceptance.
Things Not to Do:
Misconceptions
- One common misconception is that the Louisiana Medicaid Freedom of Choice (FOC) List form is only for providers who are new to Medicaid. However, both new and existing providers need to use the form to update their information, add or remove services, and ensure they're correctly listed for waiver services.
- Many believe the FOC list is automatically updated with provider information changes. In truth, providers are responsible for notifying the Louisiana Department of Health (LDH) about any changes within ten days to avoid being removed from the list.
- There's a misconception that completing the FOC form is the only step required to maintain active status. Providers must also keep their license and Medicaid provider enrollment up to date and submit these documents with the FOC form.
- Some providers think that the FOC form will notify DXC Provider Enrollment or Licensing about changes. This is incorrect; the form only updates information for the LDH Waiver Supports and Services.
- It's often assumed that the FOC form is relevant only to medical professionals. Non-medical service providers, such as those offering day habilitation or environmental modifications, also need to use the form.
- Another misconception is that the form covers all Medicaid services. In reality, it's specifically for waiver services, such as Children's Choice, NOW, and ROW waivers, and does not apply to all Medicaid-covered services.
- Some think that if they select a region for service provision on the form, they are restricted to serving only that region. Providers can select multiple regions to offer services in, as long as they're eligible and capable of serving those areas.
- There's a belief that e-mail communication is not a crucial part of the FOC form. Providing an up-to-date email address ensures important communications from LDH are received promptly.
- Many providers mistakenly believe that once they're on the FOC list, they do not need to reapply unless their services change. Regular updates and confirmation of details are essential to remain on the list, even if services offered do not change.
- Lastly, it's often misunderstood that the FOC form is a one-time submission. Providers must submit the form anytime there is a change in their services, contact information, or provider status, alongside relevant supporting documents.
Key takeaways
When filling out the Louisiana Medicaid Freedom of Choice List form for waiver services, it's important to ensure that all requested information is provided clearly and accurately. Here are five key takeaways to assist in the process:
- Make sure to print or type all requested information regarding current and former provider details. This includes names, addresses, contact names, and communication details (phone, fax, toll-free numbers, and email addresses).
- Clearly indicate the request to place, update, or remove the agency from the Freedom of Choice (FOC) list for specific provider types and regions. Check all applicable service boxes that relate to the provider's offerings.
- The form requires the provider's signature and title along with the date to authenticate the information provided. This step is crucial for the submission to be processed.
- Providers are responsible for notifying the Louisiana Department of Health, Waiver Supports and Services, of any changes in the information provided within ten days of the change. This proactive communication is essential to prevent removal from the FOC list, as keeping a provider’s license and enrollment current is mandatory.
- Submissions must include the completed FOC Form, a copy of the current license, and a copy of the current Medicaid Provider Enrollment Letter(s). These documents can be mailed or faxed to the specified addresses, ensuring that the submission is complete and can be processed without delay.
By adhering to these guidelines, providers can effectively manage their listing on the Louisiana Medicaid Freedom of Choice List, ensuring that they remain in good standing and able to offer services to Medicaid recipients.
Popular PDF Templates
La Tax Forms - A form used by qualified vehicle lessors in Louisiana to certify tax exemption on purchased vehicles for leasing.
Louisiana State Income Tax Forms - Provides a platform for individuals to report earnings not captured on a federal return, ensuring comprehensive income reporting.